Chemical properties
Drospirenone - what is it? This substance belongs to the group of oral contraceptives. Most often it is used in combination with other hormones. The drug can have a therapeutic effect on androgen-dependent diseases .
Drospirenone - what kind of hormone is it? Drospirenone is a synthetic hormone, its properties are close to natural progesterone , a derivative of spironolactone . Molecular mass of chemical compound = 366.5 grams per mole. Density of the substance = 1.26 grams per cm3, melting point is approximately 200 degrees Celsius.
Drospirenone is mentioned on Wikipedia in articles about hormonal contraception and the effect of drugs on human sexual function.
Pharmacodynamics and pharmacokinetics
Due to the fact that this substance has pronounced antiandrogenic properties, it has a beneficial effect on the course of androgen-dependent diseases such as acne , alopecia and seborrhea . Drospirenone stimulates the excretion of sodium ions and other fluids from the body, as a result of which blood pressure normalizes, swelling and tenderness in the mammary glands subsides, and body weight decreases.
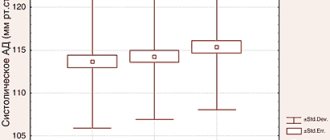
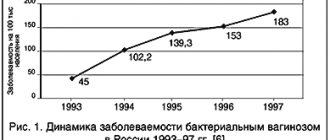
Clinical studies have shown that after 4 months of using the drug, systolic pressure decreases by an average of 2-4 mm Hg, and diastolic pressure by 1-3 mm Hg. Art., weight decreases by 1-2 kg. During menopause, women are significantly less likely to develop colon cancer , hyperplasia , and endometrial cancer .
The synthetic hormone does not have estrogenic , androgenic and glucocorticosteroid activity , does not change insulin resistance and the body's response to glucose . During treatment with the drug, the patient's blood cholesterol LDL , and the concentration of triglycerides .
After taking tablets containing Drospirenone, the active substance is quickly and almost completely absorbed by the body. The biological availability of the substance is about 75-85%. Concurrent food intake does not affect the pharmacokinetics of the drug . The concentration of the drug in the blood plasma decreases in two phases, the half-life is 35-40 hours. With systematic, daily use, the equilibrium concentration of the drug is observed after 10 days.
The product has a high degree of binding to plasma proteins (serum albumin ) - about 95-97%. The main metabolites of the hormone are formed without affecting the cytochrome P450 system . The drug is excreted in the form of metabolites in feces and urine, a small part is excreted unchanged.
Experience with the use of drospirenone-containing hormonal contraceptives
Gevorkyan M.A., Manukhin I.B., Tikhomirov A.L., Kuznetsova E.M.
Family planning has been an important medical and social problem for many decades. In Russia, this issue is most acute, since the number of abortions continues to remain high. Every second abortion (even without complications) subsequently leads to infertility, which significantly reduces the reproductive potential of the nation. This is especially true for adolescence, when the function of the reproductive system has not yet formed. It is known that the period of puberty is critical in a woman’s life and the influence of various factors (in particular, termination of pregnancy) contributes to disorders of ovarian function and endocrine infertility.
Of all the methods of preventing unwanted pregnancy, the most reliable is the use of oral contraceptives (OCs). The use of intrauterine contraceptives, especially in nulliparous young women, is undesirable due to the risk of developing inflammatory diseases of the pelvic organs and tubal infertility. In recent years, more and more women in Russia prefer OK. In large cities, the number of OK users is up to 15%. And this is undoubtedly due to the improvement of drugs that have minimal side effects. The main reason for both reluctance to take OCs and cessation of their further use is weight gain. In addition, reasons to stop taking OCs include pain in the mammary glands (mastalgia), mood changes, and headaches. All these side effects are mainly caused by estrogens and are aggravated by the progestogen component, so the search for a progestogen that would be as close as possible to endogenous progesterone in properties has continued for decades.
Drospirenone is a new progestogen included in the monophasic OK Midiana (). Drospirenone is a spirolactone analogue and has antimineralocorticoid effects, whereby it prevents estrogen symptoms associated with sodium retention, clinically manifested by weight gain, edema and mastalgia. This is a very important advantage of Midiana, which allows it to be used for PMS (premenstrual syndrome), the symptoms of which can be observed in more than 50% of women of reproductive age.
In addition, being a derivative of spirolactone (which has long been known as a peripheral androgen receptor blocker), drospirenone is effective in the treatment of dermatological manifestations of hyperandrogenism, especially acne. It is known that all estrogen-containing OCs have an antiandrogenic effect, which is based on an increase in the concentration of sex steroid binding globulins (SGBS) in the blood, resulting in a decrease in the free (biologically active) fraction of androgens. However, most progestogens of the previous generation neutralized these effects. Drospirenone does not affect the estrogen-induced increase in GSPC levels in the blood. These antiandrogenic effects of drospirenone provide women with additional non-contraceptive benefits.
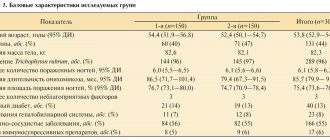
To determine the effectiveness and side effects of the new OC Midiana, our study included 54 women aged 16–40 years (average age 26±1.6)), of which 34 were “switched” from other OCs and 20 were starting to use OCs for the first time . The drug was used for 6 cycles (total 324 cycles). Taking into account our extensive experience, to reduce the frequency of acyclic bleeding in those using OCs for the first time, it was recommended to use the drug from the 5th to the 25th day of the cycle with additional barrier contraception in the 1st cycle.
During the observation process, contraceptive reliability was assessed, which was 100%, which may be due to the short duration of observation (6 cycles). In addition, the nature of side effects was assessed, the frequency of which was higher in novice users.
Acyclic bleeding was not observed in 96% of cycles. In 3.7% of cycles, spotting was observed in cycles 1–2; the frequency of cycles with breakthrough bleeding was only 0.3%. Only one woman (from beginners) refused to continue taking OCs due to these side effects.
Weight gain (minor, 1–2 kg) was observed in 5 women (9.3%), mostly novice users of OCs, which can most likely be explained by the estrogenic component of OCs. However, this was not a reason to stop taking the drug. These women were satisfied with the additional benefits of Midiana, in particular the regression of acne. Of interest are 28% of women (all of whom “switched” from other OCs) who noted weight loss on the background of Midiana, which is associated with the antimineralocorticoid effect of drospirenone.
Soreness of the mammary glands (mastalgia) was noted by 3 women (5.6%) - all of them started taking OCs for the first time. These effects are also more related to the estrogen component and stopped on the 4th cycle, i.e. optimal time to get used to OK.
Headaches were noted by 11% of women in the first 2 cycles, of which mainly novice OC users. Symptomatic medications stopped these effects, and women continued to take OCs.
Mood changes and nausea were also noted in a small number of women (1.9 and 3.7%, respectively) in the novice user group. It should be noted that women who complained of nausea had a history of dysfunction of the gastrointestinal tract or intestinal dysbiosis after the use of antibacterial drugs. These side effects were observed within 1–3 cycles and were not a reason for refusing further use of OK Midiana.
It should be noted that there was a combination of several side effects in one woman, so the total number of women presenting various complaints is significantly less.
Thus, the low incidence of side effects (11%) while taking the new OC Midiana indicates its good tolerability and high contraceptive effectiveness, which is due to the progestogen (drospirenone), which is as close in structure as possible to endogenous progesterone. This conclusion is also confirmed by the fact that only one woman (1.9%) refused to use OCs due to ongoing breakthrough bleeding. Moreover, acyclic bleeding is observed against the background of any OC.
As noted, OCs of the 21st century have additional advantages, in particular, a positive effect on the condition of the skin and symptoms of PMS, which have a negative effect on the psycho-emotional sphere, reducing the quality of life. Therefore, based on the properties of drospirenone, the effect of OK Midiana on skin condition (acne) and PMS symptoms is of interest.
Effect of OK Midiana on skin condition. Of the 54 women included in the study, 29 took OCs not only for contraception, but also for the treatment of acne. These are mainly young girls aged 16–23 who have not given birth. The choice of OCs in this group of women requires special caution, since long-term use of OCs can lead to a syndrome of hyperinhibition of the gonadotropic function of the pituitary gland. Progestogens close to endogenous progesterone (drospirenone) in OCs have the least pronounced antigonadotropic effect, which is confirmed by our data from ultrasound monitoring of folliculogenesis, which revealed normal follicular growth in 25% of women. The contraceptive effect of the drug is based on the level of suppression of the ovulatory peak of gonadotropins, and to a greater extent - atrophic processes in the endometrium. For the treatment of acne, OK Diane-35 was successfully used for a long time. However, in overweight women it promoted weight gain. 9 women who switched to Midiana not only noted an improvement in their skin condition, but also a decrease in body weight by 2–3 kg.
Effectiveness of treating PMS symptoms. Of the 54 women examined, PMS symptoms were detected in 19. The age of these women was on average 34.5 years, i.e. more senior. At this age, the incidence of metabolic syndrome and other extragenital diseases increases, which requires choosing the safest OC, which includes Midiana. Moreover, in a heterogeneous PMS clinic, there are always symptoms associated with fluid retention (edema, mastodynia), which limited the use of previous generation OCs. The antimineralocorticoid effect of drospirenone opens up new possibilities in the treatment of PMS, observed in the majority of ovulating women of reproductive age. According to the results of this study, after only 3 cycles there was a positive trend in the regression of PMS symptoms, and after 6 cycles all women noted a significant improvement and agreed to continue taking Midiana.
Thus, based on the results of the study and the existing works of foreign authors, we can conclude that the new OK Midiana is a highly effective contraceptive; contains a new progestogen drospirenone, which is as close as possible to endogenous progesterone, and has antimineralocorticoid and antiandrogenic effects. It is drospirenone that promotes stable weight, good tolerability with minimal side effects. Additional benefits - reduction of symptoms of PMS and acne make OK Midiana the drug of first choice today.
Literature
1. Guide to contraception. Edited by V.N. Prilepskaya. M. 2006.
2. Manukhin I.B., Tumilovich L.G., Gevorkyan M.A. Clinical lectures on gynecological endocrinology. M. Geotarmedia. 2009.
3. J.Verchaeghe. Hormonal contraception in women with metabolic syndrome. Contraception Reproductive Health Care. 2010. 5 (5); 305–314.
4. A. Motivala, B. Pitt. Drospirenone fore Oral Contraception and Hormone Replacement Therapy. Drugs. 2007; 7 (5): 47–655.
5. U. Halbreich, T. Backstrom et all. Clinical diagnostic criteria for premenstrual syndrome and guidelines for research studies. Genecolodical Endocrinology. 2007; 23(3); 123–130.
6. G. Paul, C. Bell et al. The real deal: A feasibility study of peer–led sex education for early school leavers. Contraception Reproductive Health Care. 2010. 5 (5); 343–357.
Indications for use
The drug is prescribed:
- as part of complex therapy for the prevention of postmenopausal osteoporosis ;
- if it is necessary to carry out hormonal contraception in women with folate or fluid retention in the body;
- as a hormonal replacement treatment for menopausal disorders to eliminate hot flashes , sweating and other vasomotor symptoms;
- with involutional changes in the genitourinary tract in women with an unremoved uterus;
- in combination with other synthetic hormones for contraception;
- for contraception in severe PMS ;
- for severe and moderate forms of acne for contraception.
Contraindications
The medicine is contraindicated:
- patients with allergies to Drospirenone;
- with porphyria ;
- persons with a tendency to form blood clots ;
- with severe liver failure;
- during lactation;
- with thromboembolism or thrombophlebitis in severe form;
- if the patient experiences vaginal bleeding of unknown origin;
- for cancer of the breast or other genital organs;
- pregnant women.
Side effects
During treatment with the drug, the following may develop:
- allergic reactions of varying severity, dizziness;
- thromboembolism of the pulmonary artery or cerebral vessels;
- thrombophlebitis , blood clots in the retinal veins;
- arterial hypertension , swelling, headaches;
- calculous cholecystitis;
- drowsiness , apathy , depression ;
- decreased visual acuity, vomiting, height or weight loss;
- galactorrhea , nausea, hirsutism ;
- alopecia , pain and swelling of the mammary glands;
- bloody or unusual vaginal discharge;
- decreased sexual desire, chloasma ;
- insomnia , decreased seizure threshold, varicose veins .
Interaction
Long-term treatment with drugs that induce liver enzymes ( barbiturates , carbamazepine , oscarbazepine , derivatives , primidone , rifampicin , topiramate , griseofulvin , felbamate ) increases the clearance of this substance and reduces their effectiveness. As a rule, this effect manifests itself 2-3 weeks after the start of therapy and persists for a month after stopping the medication.
The medicine reduces the effectiveness of drugs that stimulate uterine smooth muscle and anabolic steroids .
Vidora tablet p/o film 3mg+0.03mg 28 pcs (21+7)
Orally, whole, without chewing, with a small amount of water, 1 tablet per day, in the order indicated on the blister, starting with active tablets (21 yellow tablets) and ending with placebo tablets (7 white tablets), preferably at the same time same time of day, continuously for 28 days. When taking inactive tablets (placebo, white tablets), menstrual-like bleeding is observed. It usually begins 2-3 days after taking the last active tablet and may not end until you start taking tablets from a new pack. Taking the drug from each subsequent package begins without interruption the next day, as soon as the tablets in the previous package run out. If you have not taken any hormonal contraceptives in the previous month, you should start taking Vidora® on the first day of the menstrual cycle (on the first day of menstrual bleeding). It is possible to start taking it on days 2-5 of the menstrual cycle, but in this case it is recommended to additionally use a barrier method of contraception during the first 7 days of taking tablets from the first package. Switching from another combined hormonal contraceptive (COC, vaginal ring or transdermal patch) It is preferable to start taking the drug the day after taking the last active tablet/dragée, but no later than the next day after the usual 7-day break in taking (for drugs containing 21 tablets/dragées) or after taking the last inactive tablet/dragée (for drugs containing 28 tablets/ dragee in packaging). Taking Vidora® tablets should begin on the day the vaginal ring or patch is removed, but no later than the day when a new ring or patch is to be inserted
Switching from hormonal contraceptives containing only gestagens (“mini-pills”, injection forms, subcutaneous implants and intrauterine systems with controlled release of gestagen) When switching from the “mini-pill”, you can start taking the drug on any day (without a break), from the implant or an intrauterine system with gestagen - on the day of removal of the implant or intrauterine system, with an injection form - from the day when the next injection should have been given. In all cases, it is necessary to additionally use a barrier method of contraception during the first 7 days of taking Vidor® tablets.
After an abortion in the first trimester of pregnancy
You can start taking the drug immediately. If this condition is met, there is no need for additional contraceptive protection.
After childbirth or abortion in the second trimester of pregnancy
It is recommended to start taking the drug 21-28 days after birth, in the absence of breastfeeding or abortion. If use is started later, it is necessary to use an additional barrier method of contraception during the first 7 days of taking Vidora® tablets. If you have sexual intercourse, pregnancy should be excluded before starting to take the drug or you must wait until your first menstruation.
Taking missed inactive tablets (placebo) If you miss placebo tablets (white tablets from the last row of the blister pack), no action is required. Untaken tablets should be discarded to avoid inadvertently prolonging the period of taking placebo tablets.
Taking missed active tablets
If you miss taking active (yellow) pills and the delay in taking the next pill is less than 12 hours, contraceptive protection is not reduced. The missed tablet should be taken as soon as possible. Then the tablets should be taken as usual. If the delay in taking the next pill is more than 12 hours (the interval since taking the last pill is more than 36 hours), contraceptive protection may be reduced. The more tablets are missed in a row, and the closer this omission is to the 7-day break in taking the drug, the higher the likelihood of pregnancy, since 7 days of continuous use of the drug are required to achieve adequate suppression of the hypothalamic-pituitary-ovarian system. For such situations, the following recommendations can be given:
At 1 week of taking the drug
A missed pill should be taken as soon as possible (as soon as the woman remembers), even if this means taking two pills at the same time. Then the tablets should be taken as usual. Additionally, a barrier method of contraception must be used for the next 7 days. If sexual intercourse took place within a week before missing the next pill, the likelihood of pregnancy must be taken into account.
At 2 weeks of taking the drug
A missed pill should be taken as soon as possible (as soon as the woman remembers), even if this means taking two pills at the same time. Then the tablets should be taken as usual. If during the 7 days preceding the first missed dose, all tablets are taken correctly, there is no need to use additional contraceptive measures. Otherwise, as well as in case of missing two or more tablets, it is necessary to use an additional barrier method of contraception for the next 7 days.
At 3 weeks of taking the drug
If you miss a dose in the 3rd week, you must take the last missed tablet as soon as possible (even if this means taking 2 tablets at the same time). If you miss tablets, do not take more than two active tablets in one day. Then the tablets should be taken as usual until the active tablets in the package run out. Inactive tablets should be thrown away and tablets from the next pack should be started immediately, i.e. nonstop. Additionally, a barrier method of contraception must be used for the next 7 days. Most likely, there will be no “withdrawal” bleeding until the end of the second package, but “spotting” or “withdrawal” uterine bleeding may be observed on the days of taking the drug from the second package. If a woman has missed taking active pills, and “withdrawal” bleeding has not occurred while taking inactive pills, it is necessary to exclude pregnancy
Recommendations for gastrointestinal disorders
In severe gastrointestinal disorders, absorption may be incomplete, so additional contraceptive measures should be taken. If vomiting or diarrhea occurs within 4 hours after taking the active (yellow) tablet, you should follow the recommendations for skipping tablets. If a woman does not want to change her usual dosing regimen and postpone the onset of menstrual bleeding to another day of the week, an additional active tablet should be taken from a different package.
Changing the day of the onset of menstrual bleeding
To delay the onset of menstrual bleeding, a woman should continue taking tablets from the next package of Vidora®, skipping the inactive tablets from the current package. Thus, the cycle of taking the drug can be extended, if desired, for any period until the active tablets from the second package run out. While taking the drug from the second package, a woman may experience discharge or “breakthrough” uterine bleeding. Regular use of Vidora® is resumed after stopping taking inactive tablets. To postpone the onset of menstrual bleeding to another day of the week, a woman should reduce the duration of taking inactive pills by the desired number of days. The shorter the interval, the higher the risk that she will not have “withdrawal” bleeding, and in the future there will be “spotting” and “breakthrough” bleeding while taking pills from the second package
Additional information on use in special clinical groups
Use in children. Vidora® is indicated only after menarche. Available data do not suggest dose adjustment in this group of patients.
Use in old age. Vidora® is not indicated after menopause.
Use for liver dysfunction. Vidora® is contraindicated in women with severe liver disease until liver function tests have returned to normal.
Use for renal impairment. Vidora® is contraindicated in women with severe renal impairment.
special instructions
A number of uncontrolled randomized studies have revealed an increased risk of venous thromboembolism during treatment with the drug. It is necessary to prescribe the drug with special caution to women who have a predisposition to the occurrence of venous thromboembolism (heredity, obesity , age). It is necessary to carefully compare the risk-benefit indicators.
Rarely during treatment did benign, and even more rarely, malignant liver tumors . If the patient has any signs of this disease, pain in the area under the ribs, organ enlargement and intra-abdominal bleeding, then treatment must be interrupted.
In patients with moderate to mild renal failure, taking this synthetic hormone may affect the concentration of potassium ions in the blood serum. There is a small risk of developing hyperkalemia , especially if the patient is additionally taking potassium-sparing medications .
Before starting treatment with the drug, it is recommended to undergo a gynecological and general medical examination, it is recommended to pay special attention to the cytological examination of the ecclesiastical mucus and mammary glands, the blood coagulation system, and to exclude pregnancy. During therapy, these studies should be repeated periodically.
Drospirenone
Pharmacokinetics
After oral administration, drospirenone is absorbed quickly and almost completely. The Cmax of the active substance in the blood serum is 38 ng/ml and is achieved 1-2 hours after a single dose. Bioavailability is 76-85%. Concomitant food intake does not affect the bioavailability of drospirenone.
Drospirenone binds to serum albumin and does not bind to sex hormone binding globulin (SHBG) or corticoid binding globulin (CBG). Only 3-5% of total serum concentrations of drospirenone exist as free steroids. The ethinyl estradiol-induced increase in SHBG does not affect the binding of drospirenone to serum proteins. The average apparent Vd of drospirenone is 3.7±1.2 l/kg.
During one cycle of treatment, Cssmax of drospirenone in blood plasma is about 70 ng/ml, achieved after 8 days of treatment. Serum concentrations of drospirenone increase approximately 3-fold due to the ratio of final T1/2 and dosing interval.
After oral administration, drospirenone undergoes extensive metabolism. The main metabolites in the blood plasma are the acid form of drospirenone, formed during the opening of the lactone ring, and 4,5-dihydro-drospirenone-3-sulfate, both formed without the participation of the P450 system. Drospirenone is slightly metabolized by CYP3A4 and is capable of inhibiting this enzyme, as well as CYP1A1, CYP2C9 and CYP2C19 in vitro.
T1/2 of drospirenone with a corresponding decrease in its concentration in the blood serum after oral administration is 31 hours. The renal clearance of drospirenone metabolites in the blood serum is 1.5 ± 0.2 ml/min/kg. Drospirenone is excreted only in trace amounts unchanged. Drospirenone metabolites are excreted through the intestines and kidneys in a ratio of about 1.2:1.4. T1/2 of metabolites by the kidneys and through the intestines is about 40 hours.
Css of drospirenone in blood plasma in women with mild renal failure (creatinine clearance 50-80 ml/min) was comparable to the corresponding values in women with normal renal function. In women with moderate renal failure (creatinine clearance 30-50 ml/min), the plasma concentration of drospirenone was on average 37% higher than in women with normal renal function. Drospirenone therapy was well tolerated in women with mild to moderate renal impairment. Taking drospirenone did not have a clinically significant effect on serum potassium levels.
In a single-dose study, oral clearance in volunteers with moderate hepatic impairment was reduced by approximately 50% compared with subjects with normal hepatic function. The observed decrease in drospirenone clearance in volunteers with moderate hepatic impairment does not lead to any significant differences in serum potassium levels. Even with diabetes mellitus and concomitant use of spironolactone (two factors that can provoke hyperkalemia in the patient), there was no increase in serum potassium above the ULN. It can be concluded that drospirenone is well tolerated by patients with mild to moderate hepatic impairment (Child-Pugh class B).
Drugs containing (Analogs)
Level 4 ATX code matches:
Trisequence
Silhouette
Angelique
Divina
Claira
Hormone Drospirenone in contraceptives: Angelique , Angelique Micro (with estradiol ); Yarina , Dayla , Midiana , Dimia , Jess , Vidora , Modell Pro , Simitsia , Modell Trend (+ ethinyl estradiol ); Yarina Plus , Jess Plus (+ ethinyl estradiol + calcium levomefolinate ).
Gestodene or Drospirenone, which is better?
Both synthetic hormones belong to the latest generation of drugs. They are quite effective and have minimal side effects. Medicines containing Gestodene are more often prescribed for dysmenorrhea and to establish a regular menstrual cycle. Drospirenone is advisable to use for contraception to reduce the severity of PMS , get rid of acne , and remove excess fluid from the body. It is necessary to remember the increased risk of thromboembolism and hyperkalemia during treatment with Drospirenone.
Desogestrel or Drospirenone, which is better?
Desogestrel, like Drospirenone, belongs to the latest generation of hormonal contraceptives. By analogy with Gestodene, the substance is used to eliminate dysmenorrhea . It should also be noted that clinical studies have found that the risk of weight gain is higher during treatment with Drospirenone. In any case, the decision about which of the substances listed above should be chosen must be made by the attending physician.
Today, hormonal contraception is not only a means of preventing unplanned pregnancy, but also an effective method of treating gynecological diseases. This became possible due to the fact that in modern combination drugs the dose of hormonal components has been significantly reduced, progestogens have been synthesized with high selectivity for progesterone receptors, new routes of hormone administration have been developed, the duration and frequency of application regimens have been changed, etc., which provides a real opportunity for individualization of treatment. The use of modern contraceptives, especially hormonal ones, by women who do not need them is today not only a new chapter in the history of contraception, but also a new direction in gynecology (David Serfaty, 2011).
Intensive research and development in the field of hormonal contraception over recent years has seemingly made further improvements in hormonal contraceptives impossible. It should be emphasized that the contraceptive effect of hormonal drugs is mainly due to the action of progestogens; estrogens only potentiate the inhibitory effect of progestogens on ovulation at the level of the hypothalamic-pituitary-ovarian system.
Thus, focusing primarily on the additional non-contraceptive effects of progestogens, scientists in 1980 developed the progestogen dienogest, which does not contain an ethynyl group at position 17α, which combines the advantages of progesterone derivatives and 19-norsteroids, and in 2000 a completely new progestogen , which is a derivative of spironolactone, is drospirenone [1].
Currently, a wide variety of progestogens have been synthesized, which opens up wide opportunities for individual selection of hormonal drugs. Progestogens are steroid hormones. According to the chemical classification, they are divided into progesterone derivatives (chloramdinone acetate, medroxyprogesterone acetate, cyproterone acetate), 19-nortestosterone derivatives, subdivided into estranes (noretinodrel, norethinodrone, ethynodiol diacetate) and gonans (levonorgestrel, desogestrel, norgestimate, gestodene), as well as dienoge st , combining the advantages of progesterone derivatives and 19-norsteroids, and spironolactone derivatives (drospirenone) [2]. Progesterone derivatives do not have a contraceptive effect when taken orally.
The mechanism of action of progestogens is associated with the effect on steroid receptors. There are five types of steroid receptors: for glucocorticoids, mineralocorticoids, estrogens, progestins and androgens. Progesterone and progestogens specifically bind to gestagen receptors, but can, to one degree or another, bind to other types of steroid receptors, which determines the characteristics of their action. Thus, in addition to gestagen receptors, progesterone binds to mineralocorticoid receptors, which determines its antimineralocorticoid effect, medroxyprogesterone acetate binds to glucocorticoid receptors, so it has little glucocorticoid activity, a number of gestagens (cyproterone acetate, chloramdinone, dienogest) bind to androgen receptors [1].
Thus, the spectrum of pharmacological activity of any progestogen is determined by the severity of the gestagenic effect, the presence or absence of antiandrogenic, antiestrogenic, antimineralocorticoid activity, depending on its chemical structure.
Drospirenone is the first synthetic progestin used in combined hormonal drugs, which is not a derivative of sex steroids, but is synthesized on the basis of 17α-spironolactone and is chemically similar to the diuretic and antihypertensive drug spironolactone. Unlike other progestins, it has antimineralocorticoid and antiandrogenic activity. And its pharmacological profile is closer to endogenous progesterone than any other synthetic progestin used today. Drospirenone inhibits ovulation by suppressing the synthesis of luteinizing hormone. It also prevents fertilization by slowing the transport of sperm through changes in the cervix and cervical mucus, and prevents implantation because it causes endometrial atrophy.
Drospirenone inhibits ovulation in a dose-dependent manner. The results of a number of randomized studies conducted in healthy menstruating women indicate that the optimal oral dose of drospirenone is 3.0 mg. In these studies, the combination of drospirenone 3.0 mg and ethinyl estradiol 30 mcg completely suppressed ovulation. Like endogenous progesterone, drospirenone has an antimineralocorticoid effect on the renin-angiotensin-aldosterone system. The antimineralocorticoid activity of drospirenone 3.0 mg is comparable to that of spironolactone 25 mg, thus the antimineralocorticoid activity of drospirenone is 8 times higher than that of spironolactone.
Drospirenone and cyproterone acetate exhibit their antiandrogenic activity in therapeutic doses. Like 2.0 mg cyproterone acetate/35 mcg ethinyl estradiol, the drospirenone/ethinyl estradiol combination reduced ovarian androgen production and seborrhea in women with mild to moderate acne in a double-blind, randomized trial [3]. The antiandrogenic activity of drospirenone is about 30% of the activity of cyproterone acetate. Preclinical studies have shown that drospirenone has no estrogenic, androgenic, glucocorticoid or antiglucocorticoid activity. The special properties of the drospirenone molecule associated with the absence of an ethynyl radical, namely a more effective effect on progesterone receptors, the absence of an inhibitory effect on the liver enzymes of the cytochrome system (P450), determine its additional advantages.
A striking example is the use of drospirenone-containing drugs by patients with polycystic ovary syndrome (PCOS), a pathology of the structure and function of the ovaries, the main criteria of which are ovulatory dysfunction and hyperandrogenism. Polycystic ovary syndrome occurs in 4 to 8% of the female population of fertile age and is one of the most common endocrinopathies [4]. The syndrome is the leading cause of anovulatory infertility, skin manifestations of hyperandrogenism (hirsutism, acne), and is also associated with a high risk of developing type 2 diabetes mellitus and cardiovascular pathology [5]. However, its etiology is still unknown; therapy is symptomatic. Diagnosis of PCOS requires a differential approach and exclusion of similar nosologies. A detailed examination and identification of the main symptoms of PCOS, as well as the exclusion of clinically similar diseases are necessary to make a diagnosis.
Numerous metabolic disorders in PCOS can lead to a number of diseases, including endometrial cancer. The long-term effect of estrogen on the endometrium due to progesterone deficiency is a common cause of endometrial hyperplasia, which, if left untreated, can progress to endometrial carcinoma even in young women. Strategies to reduce the risk of cancer in PCOS include the use of combined oral contraceptives (COCs), adequate dietary counseling, weight loss, and exercise. Treatment of PCOS outside of pregnancy planning consists of correcting skin manifestations of hyperandrogenism (hirsutism, acne, alopecia), regulating the menstrual cycle, and preventing mortality from cardiovascular diseases (treatment of metabolic disorders). For PCOS in women who are not planning a pregnancy, microdosed COCs containing drospirenone are the first-line drug, since drospirenone is a metabolically neutral progestin that does not interfere with carbohydrate and fat metabolism.
Numerous studies have shown that drospirenone-containing contraceptives can be considered as well-tolerated and highly contraceptive effective (Pearl index 0.7) [6, 7]. One well-known large multicenter study involving 11 thousand women, conducted in 2004 in 15 European countries, showed a significant improvement in the overall well-being of women, which was manifested by a decrease in symptoms of fluid retention and cycle-related mood changes, as well as improvement in skin condition [8]. Another study showed a significant reduction in fluid retention and bulimia in the period preceding menstruation, as well as an improvement in mood in women by the 6th cycle of taking drospirenone-containing COCs [6].
Thus, summarizing the above data, we can highlight the following main advantages of drospirenone: • antimineralocorticoid effect (reduces sodium and water retention, as a result does not affect body weight, does not cause mastalgia and has a therapeutic effect in premenstrual syndrome); • gestagenic effect (reliable blockade of ovulation and cycle control); • antiandrogenic effect (treatment of acne and seborrhea) [9].
Today in Russia, only three drugs contain drospirenone as a progestin component: Yarina (drospirenone 3 mg, ethinyl estradiol 30 mcg), Jess (drospirenone 3 mg, ethinyl estradiol 20 mcg) and the recently registered Midiana (drospirenone 3 mg, ethinyl estradiol 30 mcg).
I would like to present the results of the use of Midiana, obtained by our colleagues and us at the Scientific Center for AGiP of the Ministry of Health of the Russian Federation. In the study by I.B. Manukhina et al. 54 women aged 16–40 years were included (mean age: 26.0 ± 1.6 years), of which 34 had previously taken other oral contraceptives (OCs) and 20 had started using OCs for the first time. The drug was used for 6 cycles (total 324 cycles). To reduce the frequency of acyclic bleeding in patients using OCs for the first time, the authors recommended using the drug from the 5th to the 25th day of the cycle with additional barrier contraception in the 1st cycle. Contraceptive reliability was 100%. In addition, the nature of side effects was assessed, the frequency of which was higher in patients who took hormonal contraception for the first time. Acyclic bleeding was noted in only 4% of cases. The rate of cycles with breakthrough bleeding was only 0.3%. An increase in body weight (by 1–2 kg) was noted in 5 (9.3%) women, mostly novice users of OCs. And in 28% of women (all of whom “switched” from other OCs), a decrease in body weight was noted while taking Midiana. The authors noted other side effects, such as mastalgia, headache, mood changes, and nausea, but these were extremely rare. All side effects resolved within the first few months of taking the drug, without having a significant impact on tolerability and adherence to treatment. Only 1 (1.9%) woman refused to use the drug due to continued breakthrough bleeding. Thus, the low incidence of side effects (11%) when taking the new drug Midiana indicates its good tolerability and high contraceptive effectiveness [10].
Our preliminary data, based on the use of Midiana by 32 women of reproductive age, indicate that the drug is well tolerated, reliable cycle control and no cases of refusal to use it. The duration of use of the drug was 6 months.
Thus, the increase in the arsenal of drospirenone-containing compounds with the introduction of the drug Midiana allows us to hope for a further expansion of the possibilities of their use in the practice of an obstetrician-gynecologist.